


Agile and Physical Health - Part 3 - Historical Data
"History is just one damn thing after another." - Morgan Housel, "The Psychology of Money"


The beginning modules in the Early Medical program emphasize the importance of good data along with solid goals for the future when working to expand healthspan and lifespan. The program stresses the importance of developing a sound strategy based on quality data before jumping into tactics. This is counter to the don't-just-stand-there-do-something reflex many people have. A fine reflex if there's a fire to be fought, but not so good when there's an elephant that needs to be removed from a room. And for complex systems like human biology, it's important to know how things got to be the way they are.
"Individuals and interactions over processes and tools" - one of the trusty Agile values from software development. No reason it couldn't or shouldn't be applied to human service domains, such as medicine. Machines and lab tests have their value, but to round out an individual's picture of health we need to know about the person, specifically. We need to interact with the actual human being and hear their story, their history. When Fate decides it's our turn to be the patient, it's important to know our history.
To know what needs to change and improve our health we must have as complete a picture as possible of our present state of health. Thousands of dollars worth of lab tests and physical examinations aren't enough to fully understand the present state. We have to also identify key patterns and events from the past that have had a significant and lasting impact on our health. Not just from our own past, but that of our ancestors as well. We are in a unique position for deep exploration into our health history, going back for as many generations for which we can find records.
The Early Medical program acknowledges that a robust family health history isn't available to many people. Perhaps they were adopted or there's no clear record. In my case, family health history lands more toward the latter. I come from a background of farmers and ranchers. They had a rudimentary working knowledge of physical health, consisting of home remedies or simply living with physical limitations. Events and causes weren't tracked or recorded.
Lifespan
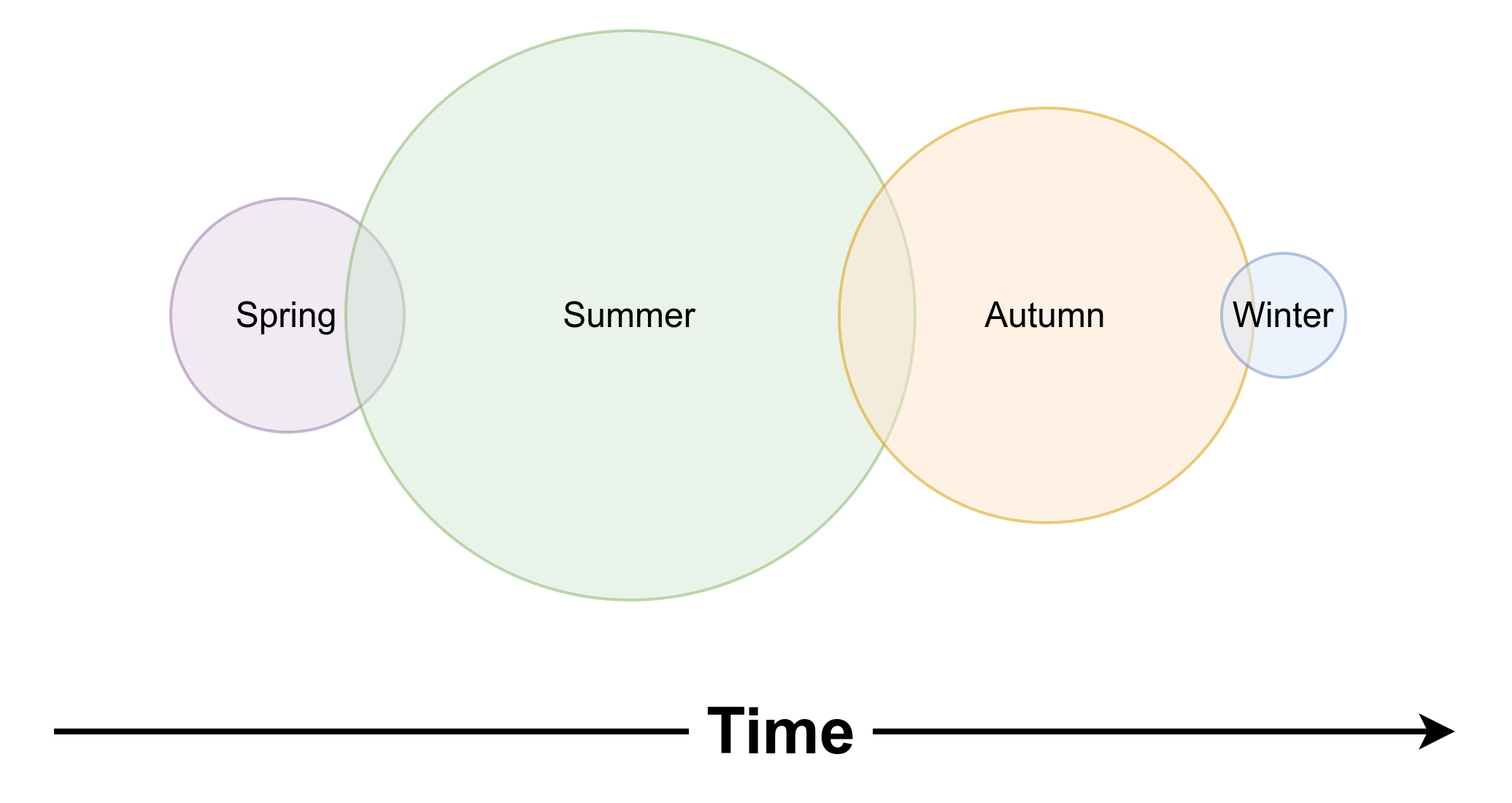
Splitting the phases of our life into "quarters" or decades belies a precision that doesn't exist in human experience. I prefer the seasons. There are days on the edges of Summer that feel like Spring or Autumn, days on the edges of Autumn that feel like Summer or Winter, and so on. There's no clear line between seasons except for the artificial demarcations on the calendar.
Unlike the steady pulse of Nature's seasons, if Fortune grants us a long-ish lifespan we each get one ride around the cycle, one iteration through the seasons of life to do with what we will. Each season adding a different dimension to the record of our days.
This exercise resulted in a mini-autobiography. Included in this post are what stand out as important to my current health and how I got here.
Spring (0 - 25 years)
The Negatives
History of familial hypertension and possible cardiac issues
Part of a large family with scarce resources. I was weaned to a diet that was quite industrial in its composition: powdered milk, Velveeta "cheese," margarine, 70% lean ground beef in a tube, and lots of pasta and rice. Fresh vegetables were infrequently found on the table and most of what we ate came from a can or frozen in a bag. It was poor quality food and there was never enough of it. Developed a strong affiliation for carbohydrates, particularly sugar.
Trusted government dietary guidelines that asserted the importance of carbohydrates over fats.
Very poor sleep habits and patterns due to a home environment saturated with fear and anxiety.
The Positives
No clear history of cardiac or neurodegenerative diseases.
Without a driver's license until I was 22 years old, to get around, I either walked or rode my bike. Didn't appreciate this at the time, but it kept me active and fit.
Summer (20 - 60 years)
The Negatives
Working the night shift for four years during my early 20's further adversely affected my sleep habits.
Working two sedentary jobs for 10 years to pay for my first wife's medical bills further adversely affected my sleep habits.
During the cancer decade, I gladly reached for comfort foods, mainly chips and ice cream, to deal with stress and anxiety. When my first wife died, I was 44 years old and weighed 245 lbs. - the heaviest I've been in my entire life.
Death of a spouse. This will factor into a subsequent post on risk assessment.
The Positives
Degrees in biochemistry and cell biology.
The ability to easily read peer reviewed research articles in any of the hard sciences.
No longer trusted government dietary guidelines.
Established a strong meditation practice that continues to this day.
The thousands of hours of Aikido practice on my way to a 3rd degree black belt rank provided vigorous physical exercise.
Autumn (55 - 80 years, My current season)
Over the years I've cobbled together a loose framework for keeping my health in order. Keeping track of changes and progress, however, is a more recent addition to my health strategy. About ten years ago I started tracking blood pressure (BP) more closely, since this is a health issue for which I'm genetically predisposed. Initially, this was tracked using an in-home BP monitor and a spreadsheet while working to control BP with diet and behavior changes. Eventually, failure to keep my BP in a healthy range through diet and behavior meant starting medication to manage it. For the past 5 years I've taken two pressure readings (morning and evening) on most days, each measurement the average of three readings on two in-home BP devices.
My attitudes and beliefs around the use of pharmaceuticals were an obstacle to making the decision to start BP medication. For about a year after college, I worked as a quality control chemist at CIBA-Geigy. The business side of the industry isn't what turned me away from pharmaceuticals. Rather, it was the idea of being reliant on something that required such elaborate manufacturing and regulatory structures to produce. What if I relied on a drug that then became unavailable or too expensive? This holds true for supplements. As much as possible, I work to support my body's natural ability to function with high quality food and clean water. These attitudes and beliefs may have been fine when I was young and healthy, but prove to be limiting in the Autumn of my life.
To track the data effectively, I wrote a database application that allows for easy data entry and analysis. It shows me ranges and averages (table, histogram, and line chart) for all the records in the past 30, 60, 90, and all days. Tracking BP data to this level revealed several important aspects of my BP profile and how to best manage it.
There's a right way and many wrong ways to take a blood pressure reading. EVERY doctor's office I've visited in my life does some version of the wrong way.
Consistent exercise helps lower my BP. There have been several stretches - usually during an active summer - where I've skipped medication for multiple days. On advice of my doctor, this was prudent as taking it would cause my BP to drop too low. I can tell when this is happening because with a BP down around 110/70, I physically don't feel good and become light headed if I stand up too fast.
It's important to track both the systolic and diastolic pressures. Early on, medication was bringing down my systolic, but not diastolic. So the medication was adjusted.
I sleep better when my BP is at or below 120/80.
My BP is almost always higher first thing in the morning than it is at the end of the day. This is natural and part of the normal process of waking up from sleep.
Alcohol causes my BP to drop by 10-15 mmHg, but I don't sleep as well and my BP is often elevated the next day.
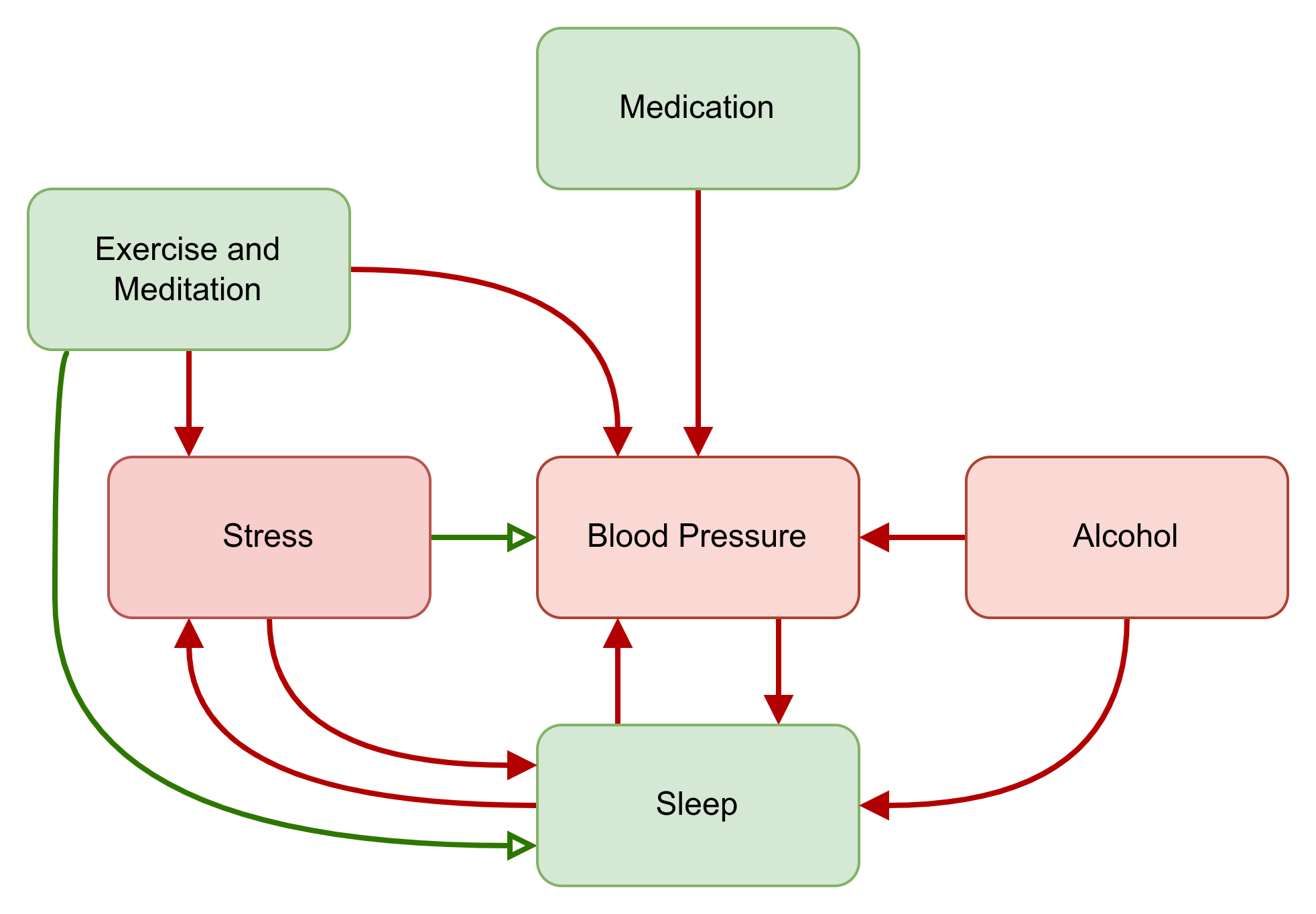
No surprise, stress causes BP to go up. But I've been able to identify specific stressors to avoid. The effect can last anywhere from several days to a week once the stressors are removed or resolved.
Through medication, diet, and behavior changes, my BP issue is well managed and controlled. Figure 1 shows the core causal loops involved with keeping everything in check.
Blood markers, however, tell a good-news/bad-news story on the cardiac and metabolic front. Since this post is dedicated to establishing history, I'll just round out what's seasonal with a few notes about information sources that have helped me stay on the pre-diabetic side of things for the past 10+ years.
The most significant shift came after reading Gary Taubes' book, "Good Calories, Bad Calories" in 2008. A lot more research has been done in the last 16 years so I'm not sure just how well Taubes' book holds up today. I'd wager his central thesis - that carbohydrates, particularly refined sugars, are a primary driver behind metabolic diseases - still holds true along with the historical information regarding the highly politicized government dietary recommendations.
Regardless, Taubes' book inspired me to dig deeper into the biochemistry and stay current with evolving research over the years. I spend a lot of time on PubMed , the Public Library of Science (PLOS), and Google scholar. In addition to aggregating my own scientific sources, I follow the podcasts from Andrew Huberman and Peter Attia. While I greatly appreciate the work each of these scientists do, I am equally grateful that each of them usually cite their sources. This added information not only builds my trust in them, but has also allowed me to pursue many interesting rabbits down into their information-rich burrows.
Winter (80+ years)
I look forward to building this bridge when I get there.
Disclaimer
The author has Bachelor degrees in both biochemistry and cell biology but is not a licensed practitioner of medicine or psychotherapy and nothing presented on this website claims or should be construed to provide medical or psychotherapeutic advice. This series of articles is presented as a personal reflection by the author on work he's done to improve his health and as such is relevant to the author and no one else. The author makes no recommendations as to any course of action the reader may chose to follow other than to encourage the reader to work closely with qualified health professionals when making healthcare decisions relevant to their personal lives.
← Agile and Physical Health - Part 2 - Goals
Agile and Physical Health - Part 4 - Empirical Data →
Related Articles



If you have any questions, need anything clarified, or have something else on your mind, please send a DM or email me directly.
Image by Heiko Stein from Pixabay